










This article is the English version of original version in Bahasa Indonesia (April 22, 2020) on the possibility of using Estrogen to reduce the death of COVID-19 - with some update of data and a trial that is ongoing in LA, USA (Source)
Summary: Although the risk of getting infected by SARS-CoV-2 does not discriminate among men and women, the number of fatality cases around the world shows the men are definitely more at risk to develop severe symptoms leading to death. Co-morbid patients both men and women are at higher risk of acquiring the virus infection due to elevated activity of enzyme ACE2 (as results of some anti hypertension medicine), furthermore risk of fatality of these group also increases.
Among the COVID-19 fatal cases due to acute respiratory distress syndrome (ARDS), immunity responses were often preceded with “cytokine storm”. While anti-cytokine drugs are in the market, e.g. tocilizumab (anti IL-6) which being studied in China (will be completed May 3, 2020), price of the medicines makes the availability limited only to certain people. High estrogen level in reproductive women responses aggressively, fast and targeted during innate immunity system responses as well proportional during adaptive immunity response, preventing cytokine storm.
Complexity of men testosterone level and immunity response is yet to be concluded, study has shown that elevated level of testosterone in men resulted lower antibody level acquired following the flu-vaccine shot, on the other hand strong responses were observed in women and men with lower level of testosterone.
The Estrogen (E2: estradiol) inhibits expression of pro-inflammatory cytokines in various type of cell. Women in menopause, in which the level of E2 has dropped drastically, the E1 (Estrone) takes over the function of E2 in immunosuppression. Similar repressive effect on IL-6 and other pro-inflammatory cytokines is although to be the case when phytoestrogens from dietary intake from food like soy (tempeh).
Strong and accurate immune response seen in women antigen SARS-CoV-2 is probably through E2 modulated immune response. If the estrogens are the key in preventing the cytokine storm, fatality cases due to ARDS can be reduced by increasing the level of estrogen (especially E2) from outside body by E2 hormone injection or as simple as taking birth control pills (Estrogen and Progresteron).
Regardless there are ample data showing the possibly adverse effect of the estrogens therapy, short-term use of estrogen in saving patient life outweighs the risk of developing adverse effect in the future. So, it is worth a try, at least for elderly women.
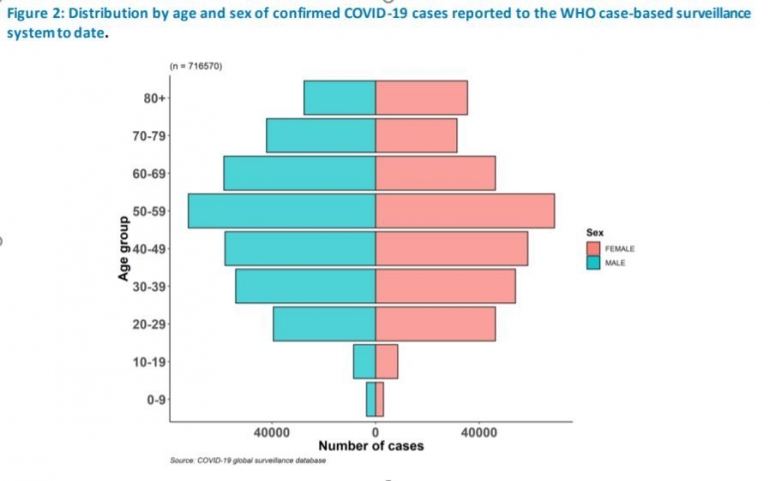
Risk of Infection. Data from various sources show that gender is not correlated with the risk of being infected with SARS-CoV-2. However, patients with COVID - 19 who ended fatally were more on male patients who were> 60 years old. The risk of infection and death becomes greater if SARS-Co-V-2 infects comorbid patients both male and female, e.g. patients with diabetes, high blood pressure, heart disease, asthma and other degenerative diseases.
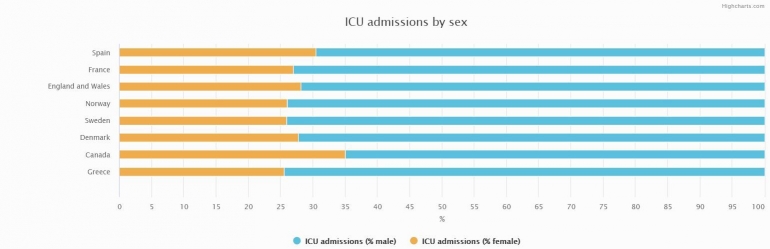
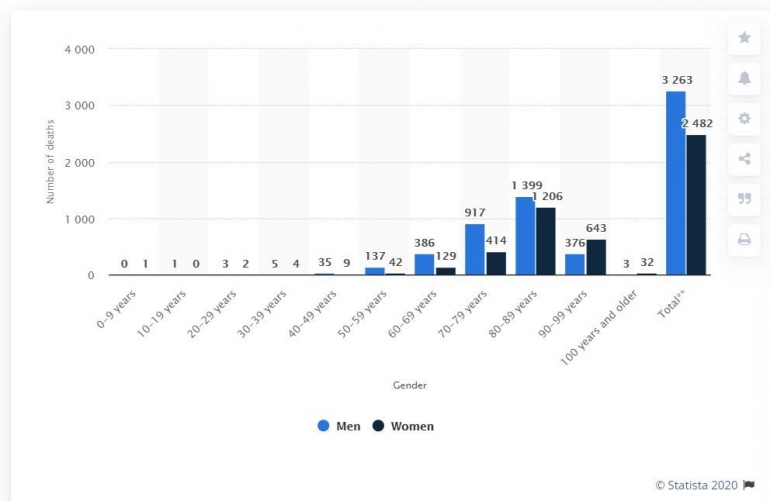
Finally, data from the most severely affected areas in Italy, Lombardy, showed that 82% of patients entering ICU were male and 70% of COVID-19 deaths were male. Data from USA, male-female segregated data is only the City of New York, as of April 14, 2020, the largest number of deaths was in patients older than 75 years (48%), then 25% for the age range 65-74 years and 23% for the range 45 -64 years old.
However, if the number of deaths of 6,839 were seen from the sex, the death of male patients reached 62% and 38% of women. The chart below shows the percentage of deaths of male patients of COVID-19 in various countries which is always greater than female patients, although the percentage of cases in men in some countries is lower than women. https://globalhealth5050.org/covid19/#1586248980572-3839d9fe-3b88
Death of a Male COVID-19 Patient. So what causes male patients to have a greater fatal risk, data from China say that large male patient deaths is due to most men in China, which based on national statistics are smokers (50% of men vs. 5% of women, this is because in Chinese culture, there is a negative stigma against women who smoke).
As well as Italy, where male smokers are 25% more than women. However, this trend is not found in Spain, which according to national statistics the number of male and female smokers are only slightly different. Furthermore, for patients who are fatal in China, although further study is needed, the current conclusion is that the possibility of active smokers entering ICU (and requiring ventilators) and ending in death is 2.4 times greater in non-smokers. Source.
Role of the ACE2 Enzyme. Apart from smoking habits and sufferers with other illnesses, hormonal aspects are beginning to be investigated as factors that cause higher mortality of male patients. The dominant testosterone hormone in men is known as a hormone that can decrease the body's immune system, and it is inconsistent, where when antigens enter, there are immune cells that show an active response, some are response slow and weak, some are even not concerned about the antigens.
Conversely, estrogen in women is known as a hormone that increases a woman's immunity. When the SARS-CoV-2 virus enters through the lungs eventually reaching the alveoli (the smallest vessel in the lungs where it exchanges oxygen with carbon dioxide), with intermediate enzyme ACE2 the virus lands perfectly on the target cells, i.e. the epithelial cells in the alveoli.
Furthermore, the RNA released by the virus, helped by Trans-membrane protease serine 2 enzyme (TMPRSS2) will start hijacking the cell's work by asking the body's cells to replicate the virus.
Against this incoming antigen, the immune cell responds by releasing inflammatory cytokines (pro-inflammatory cytokines). this is to recruit white blood cells (B-Cells, T-Cells, Macrophages and Monocytes) to the source of infection to get rid of the antigens (Viruses) through various mechanisms, such as monocytes that look like kidney beans are vacuum cleaner that will eat viruses , bacteria, protozoa and others, and when these dead cells die, they will be cleansed by the body's lymphatic system.
Cytokine Storm. The release of pro-inflammatory cytokines is the body's natural response to deal with the influx of antigens such as viruses, but there are times when the body responds excessively, which causes what we know as the Cytokine Storm.
During the cytokine storm, white blood cells that are recruited or mobilized become too many and out of control by attacking and destroying healthy cells that should be protected. This cytokine storm phenomenon is one that has been widely studied since 2005 when bird flu occurred. The high mortality rate in bird flu patients is directly related to the uncontrolled cells response in the release of cytokines.
Like avian influenza caused by the H5N1 virus, SARS, MERS, SARS-CoV-2 are from the beta-corona group, in many cases the fatality of COVID-19 patients end with one or multi - organ failure resulting from cytokine storm. In the case of acute lung organ failure (Acute respiratory distress syndrome), the lungs are filled with fluid or pus due to too many dead white blood cells.
The consequences of this excessive response are fatal and generally lead to death. Research also proves that the failure of other vital organs such as kidney, liver, heart, and intestine can also be a result of the cytokine storm, so researchers hypothesize that the death of COVID-19 patients may be reduced if the cytokine storm can be inhibited.
The cytokine storm might also explain why children are "stronger" both from the risk of being infected (which is lower) and even if infected, the chance of fatality is less than that of adults.
Not only in SARS-CoV-2, in infections caused by the SARS and MERS viruses this also happens, there is no definitive answer in this case, but experts have the hypothesis that the immune system of children under 10 years is imperfect so production of pro- inflammatory cytokines are also lower. source.
Anti-cytokines Medicine. Before COVID-19, many researchers have tried to find medicines that could inhibit the cytokine storm known as cytokine blockers or anti-cytokines. From the many studies there are several medicines that have been marketed as cytokine blockers such as ustekinumab, infliximab, adalimumab and tocilizumab (these drugs are used by rheumatoid arthritis patients and other auto-immune diseases). Each of these drugs inhibits different types of pro-inflammatory cytokines, there are anti-interleukin [IL] -12 / IL-23, anti-tumor necrosis factor (TNF) and IL-6. A report by Lancet states that patients who take these drugs and are infected and become COVID-19 positive patients have not ended up in the ICU nor have acquired pneumonia. There is no further research whether the drug users above are people who are resistant to COVID-19. source.
Pneumonia caused by SARS-CoV-2 is characterized by hyper T-immune cell activation and an overproduction of pro-inflammatory cytokines, specifically IL-6. The researchers hypothesized that patients using tocilizumab would be able to control the production of IL-6 cytokines, so they might be more resistant to SARS-CoV-2. The possibility of effective anti-cytokines drugs is currently being investigated. Currently tocilizumab is being studied in China for 188 COVID-19 patients (will be completed on May 3, 2020). Other drugs that work on cytokines such as anti-TNF also receive special attention to be tested on humans immediately. source
Apart from the result that may show the anti-cytokines medicines to be effectiveness, the price of these drugs is expensive (for example tocilizumab: US $ 20-30 thousand per treatment) and the side effects that can result in patients exposed to bacterial and other viral infections make the above drugs become limited use.
Estrogen levels (especially E2) that are relatively high in women during reproduction to pre-menopause age help the formation of an aggressive immune system (jump-start - innate immune response) and effective. In other words, the response of immune cells when dealing with antigens such as viruses is massive, very fast and precise during innate immune response.
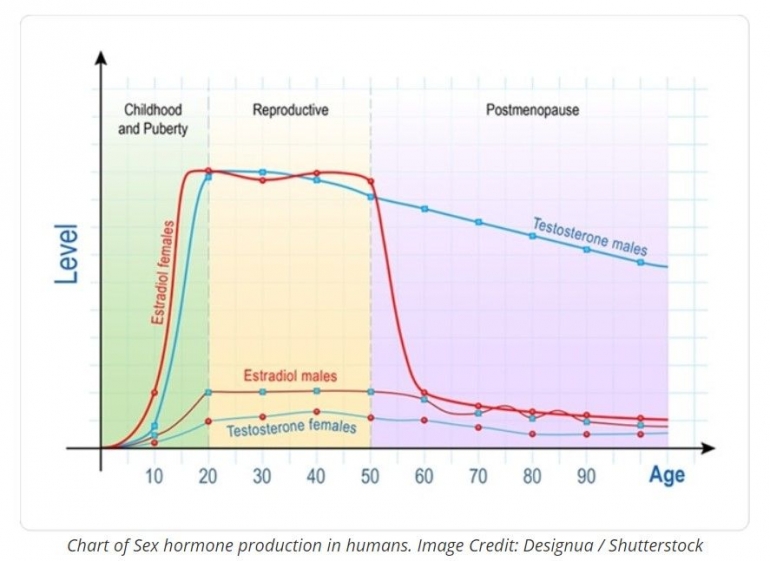
Estrogen levels of women during reproduction age also control that the response to antigens is proportional during the adaptive immune system works, not excessive that can lead to cytokine storm. The graph below shows women's Estradiol levels drop dramatically when women enter post-menopause but are still higher than men until the age of 70, after that estradiol levels continue to fall with age, but then level of Estrone (E1) increase, replacing the role of E2 in post-menopause women.
Unlike estradiol, the dominant male hormone testosterone, although it decreases after reaching its peak at the age of 20 years, the decrease is not as drastic as the level of estradiol in women. Long research also explains that high testosterone levels are correlated with a low immune system response, this is evidenced that men with high testosterone levels produce less reactive antibodies when injected with influenza vaccine. Conversely, men with lower testosterone and women respond better and produce more reactive antibodies. source.
Estrogens and Pro-inflammatory Cytokines. Numerous studies have shown a complex relationship between testosterone hormone levels in men and immune cell responses that are inconsistent (sometimes "on", sometimes "off", sometimes too slow, sometimes does not matter). However, this does not happen with the female hormone estrogen.
Many studies show that the loss of the hormone estrogen in women (for example when the ovaries are removed) increases cytokine activity. Conversely, administration of estrogen (oral or injection) inhibits cytokine activity. This has been proven by many studies, treatment with estradiol (E2) inhibits IL-1β and TNF-α induced by osteoblasts-like cells, monocytes / macrophages and others. E2 also inhibits the activity of IL-6 from several cells including endothelial cells that are found in the lymphatic system and blood vessels.
As we all know IL-6 is closely related to SARS-CoV-2 infection and COVID-19 patients who end fatally due to cytokine storm which is dominated by IL-6. Serum IL-6 was found lower in post-menopausal women with hormonal replacement therapy, compared with those who did not receive hormone replacement therapy. Like E2, estrone (E1), which is the dominant estrogen in menopausal women as well as phytoestrogens such as those derived from legume such as soybeans also show an immunosuppressive effect on IL-6, just like the effects of E2. source.
Key points:
- The risk of being infected with SARS-CoV-2 is no different for men or women,
- The risk of fatal COVID-19 patients is greater for male patients,
- COVID-19 comorbid patients both men and women are more susceptible to infection (because ACE2 is more active) and the risk of fatality increases,
- The main death of COVID-19 patients is due to cytokine storms that lead to acute pulmonary failure (ARDS),
- Anti-cytokine drugs that are being tested such as tocilizumab (anti-IL-6) are still out of reach of the general public because of the high price,
- Estrogen hormone in women responds to SARS-CoV-2 infection aggressively, quickly and precisely when the natural immune response, and proportional to the adaptive immune response.
- High levels of the hormone testosterone in men can cause a weakening of the immune system; the inconsistent response to antigens in men is a complex matter that cannot be concluded at this time,
- Estrogen (E2: estradiol) in women suppresses the formation of pro-inflammatory cytokines in many cell types. In menopausal women when E2 decreases dramatically, E1 (Estrone) takes over the function of E2 in providing immunosuppression. The repressive effect on IL-6 and other pro-inflammatory cytokines may also be obtained by ingesting foods rich in phytoestrogens such as soybeans in tofu and tempeh.
Medical Hypothesis. The response of the hormone estrogen (especially E2) in women who are so aggressive, fast and precise to the SARS-CoV-2 antigen. Estrogen also controls the production of Pro-inflammatory Cytokines so that there is no fatal Cytokine Storm that can be fatal with acute lung failure (ARDS) in COVID-19 patients. Regardless estrogen is produced by the body or comes from outside the body, its effects on pro-inflammatory cytokines are the same. For this it can be hypothesized that if a COVID-19 patient (including PDP and even ODP) gets outside estrogen intake such as birth control pills, then the possibility of death for COVID-19 patients or the number of patients needing an ICU (and ventilator) will decrease. Regardless that estrogen is a double-edged sword, a reduction in the number of victims of COVID-19 is paramount and short-term estrogen therapy may not trigger the negative effects of estrogen or feminization
Baca konten-konten menarik Kompasiana langsung dari smartphone kamu. Follow channel WhatsApp Kompasiana sekarang di sini: https://whatsapp.com/channel/0029VaYjYaL4Spk7WflFYJ2H
